Health Insurance Forms & Benefits
As an employee of Mission Yogurt we are pleased to offer you a full selection of benefits. You are eligible for medical, dental, vision, and life insurance.
Important – You may enroll only at certain times
- During the annual open enrollment period, July 1st.
- First of the month following 60 days of employment.
- Change of life event within 31 days (married, divorce, have a baby, etc.)
Eligibility
- Average/Minimum of 30 Hours per Week
Summary of Benefits

July 1, 2023 – June 30, 2024 Medical (In Network Summary)
| 2024 Medical (in Network) | Copay | Health Savings Account | |
|---|---|---|---|
| Preventative / Wellness Copay | $0 | $0 | |
| Primary / Specialist Copay | $5 / $80 | 70% after deductible | |
| Urgent Care / Emergency Room Copay | $75 / $300 | 70% after deductible | |
| Prescription Drugs | $10 / $20 / $40 / 20% | 70% after deductible | |
| Deductible (individual/family) | $1,500 / $3,000 | $5,000 / $6,850 | |
| Out-of-Pocket maximum | $6,000 / $12,000 | $6,350 / $6,850 | |
| Coinsurance | 80% after deductible | 70% after deductible | |
| Outpatient Facility Deductible | $0 | $0 | |
| Out-of-Network Coverage | Yes (refer to SBC) |
|
|
| Amount Per Pay Check | |||
| Employee Only | $10.00 | $0.00 | |
| Employee + Spouse | $256.41 | $202.57 | |
| Employee + Children | $211.76 | $165.75 | |
| Employee + Family | $458.30 | $368.30 | |

July 1, 2023 – June 30, 2024 Dental (In Network Summary)
| 2024 Dental (in Network) | Basic | Enhanced |
|---|---|---|
| Cleanings 2x Per Year | $0 | $0 |
| Deductible (individual/family) | $50 / $150 | $50 / $150 |
| Basic Services | 80% | 90% |
| Major Services | 50% | 60% |
| Annual Maximum | $1,000 | $1,000 |
| Out-of-Network Coverage | Yes (reduced benefit) | Yes (90% UCR) |
| Amount Per Pay Check | ||
| Employee Only | $11.56 | $22.01 |
| Employee + Spouse | $24.00 | $45.70 |
| Employee + Children | $27.07 | $51.37 |
| Employee + Family | $41.39 | $78.57 |
July 1, 2023 – June 30, 2024 Vision (In Network Summary)
| 2024 Vision (in Network) | Basic |
|---|---|
| Exam Copay (1x every 12 months) | $10 |
| Lenses (1x every 12 months) | $25 |
| Retail Frames Allowance (1x every 12 months) | $200 |
| Covered Selection Contacts (1x every 12 months) | $200 |
| Amount Per Pay Check | |
| Employee Only | $4.13 |
| Employee + Spouse | $8.95 |
| Employee + Children | $9.79 |
| Employee + Family | $16.23 |

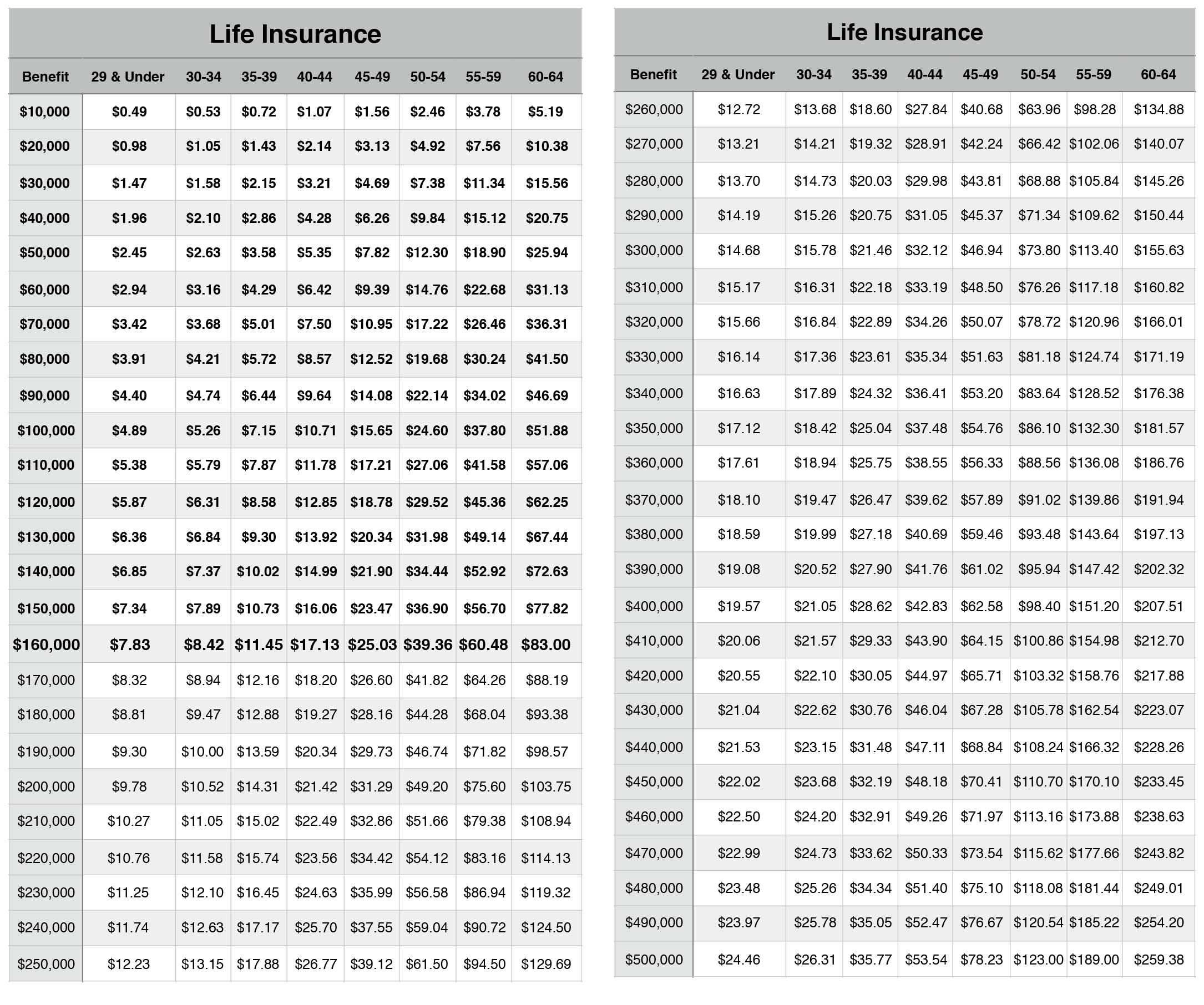
July 1, 2023 – June 30, 2024 Voluntary Term Life Benefits Summary
| Employee Life Benefits | Spouse Life Benefits | Child Life Benefits | |
|---|---|---|---|
| Benefit Amount | Choose benefits in increments of $10,000 | Choose benefits in increments of $10,000. | Generally Options are: • $10,000, or • $20,000 |
| Minimum | $10,000 | $10,000 | $10,000 |
| Maximum | $500,000 | $100,000 | $20,000 |
Guaranteed | $160,000 | $30,000 | $20,000 |
Aged based reduction: The maximum benefit for a dependent child under 6 months old is $1,000. Additionally, when you are 65 or older, your life insurance benefit will reduce to the percentages shown below.
65% of Total Benefit at Age 65
50% of Total Benefit at Age 70
Benefit Reductions will be effective on the Policy Anniversary Date coinciding with or following the Employee’s attainment of age as specified above.
Open Enrollment 2024 – Mandatory Participation
- Posters at your location indicating meeting times/dates for open enrollment
- Flyers on your check
- E-mails
- Monthly Newletters Notifications
It is important to attend to be aware of any benefit/rate changes, even if you are not enrolled in our plans.
Voluntary Term Life Insurance (In Network Summary)
Additional Employee BenefitsCoverage During DisabilityIf you become disabled before age 60, coverage will continue and premium may be waived for you and your covered dependents.Accelerated Death BenefitIf you become terminally ill, you may be able to receive a portion of your life coverage benefit as a lump sum.Individual Purchase RightsIf you terminate employment, you may be able to convert benefits to an individual policy.PortablilityIf you cease to qualify as a member, you may be able to continue coverage for you and your covered dependents.Limitations & ExclusionsSuicide ExclusionBenefits are not paid if you or your dependents commit suicide within the first 12 months of coverage (prior group voluntary life coverage applies towards the 12 month time period).Coverage Outside the USBenefits will not be paid if you or your dependents are outside the United States for certain reasons for more than six months.
Important Documents
Cigna
Welcome to Cigna
Special Enrollment Requirements
Cigna Instructions
Employee Benefits
Cigna Telehealth Connection
Medical
LocalPlus
Summary of Benefits – LocalPlus
Summary of Benefits – HSA LocalPlus
Summary of Benefits and Coverage: LocalPlus
Summary of Benefits and Coverage: HSA LocalPlus
Preventative Health Care
Know Before You Go
Cigna Medical Vaccine Program
Dental
A Guide to Your Cigna Dental PPO
Mission Yogurt, Inc. – High Plan
Mission Yogurt, Inc. – Low Plan
Vision
Cigna Vision
Summary of Benefits – Cigna Vision
Pharmacy and Drugs
Know Which Drugs are Covered Under Your Plan
Specialty Pharmacy Drug List
Your Pharmacy Benefits
Cigna Home Delivery Pharmacy
90-Day Prescription Fills