Health Insurance Forms & Benefits
As an employee of Mission Yogurt we are pleased to offer you a full selection of benefits. You are eligible for medical, dental, vision, and life insurance.
Important - You may enroll only at certain times
- During the annual open enrollment period, July 1st.
- First of the month following 60 days of employment.
- Change of life event within 31 days (married, divorce, have a baby, etc.)
Eligibility
- Average/Minimum of 30 Hours per Week
Summary of Benefits



Important Documents
- CignaWelcome to Cigna
- Health and LifeLocalPlus
Special Enrollment Requirements
Enrollment/Change Form
Employee Benefits
Cigna Telehealth Connection
Summary of Benefits - LocalPlus
Summary of Benefits - HSA LocalPlus
Summary of Benefits and Coverage: LocalPlus
Summary of Benefits and Coverage: HSA LocalPlus
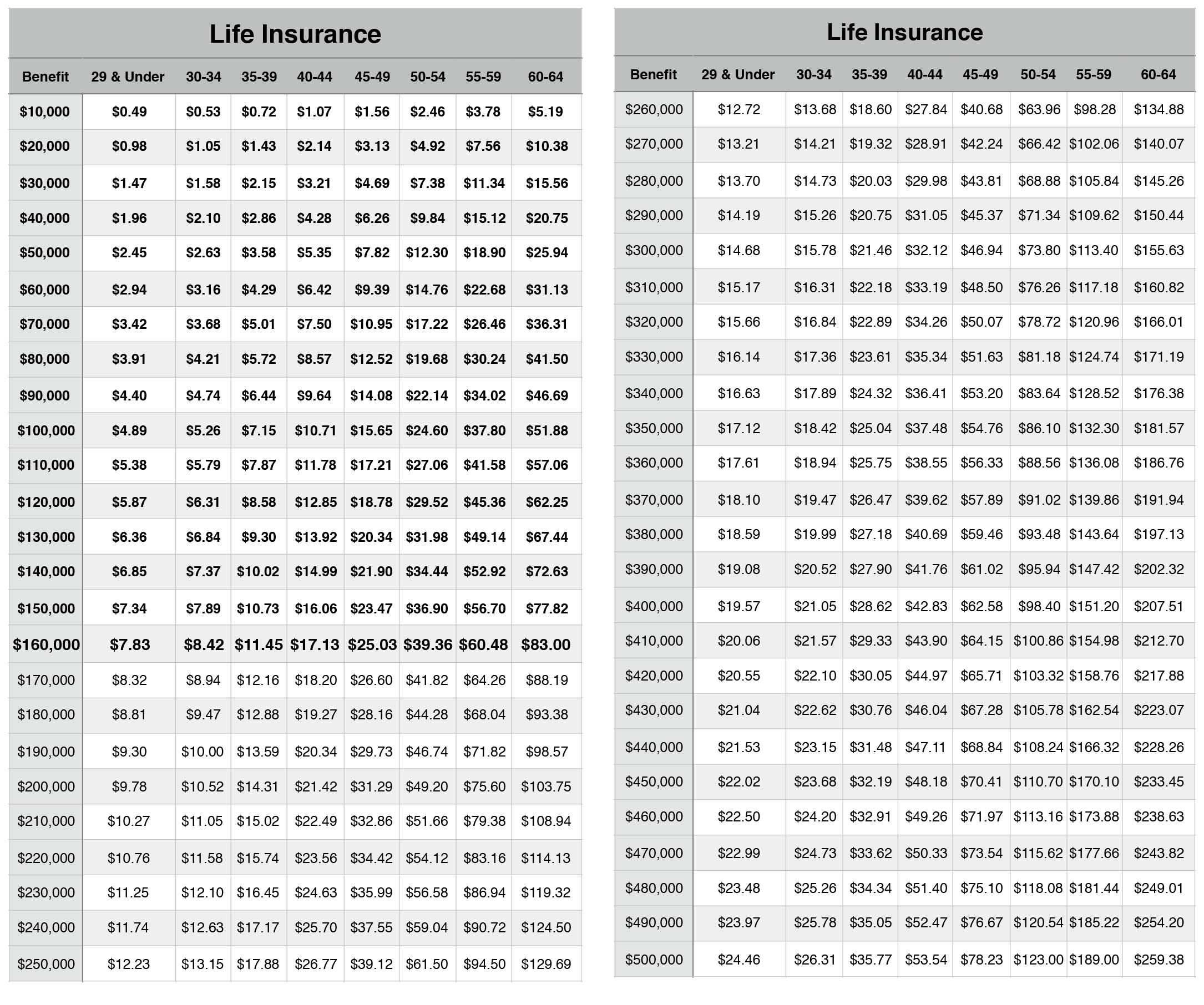
Life Insurance Application
Preventative Health Care
Know Before You Go
Cigna Medical Vaccine Program
- DentalA Guide to Your Cigna Dental PPO
- VisionCigna Vision
- Pharmacy and DrugsKnow Which Drugs are Covered Under Your Plan
Mission Yogurt, Inc. - High Plan
Mission Yogurt, Inc. - Low Plan
Summary of Benefits - Cigna Vision
Specialty Pharmacy Drug List
Your Pharmacy Benefits
Cigna Home Delivery Pharmacy
90-Day Prescription Fills